 My treatment strategy for MS stands out for its safety, efficacy, speed and low cost, compared to the standard treatments which are designed to work through the CNS, but it doesn’t impress. I don’t like the DMTs and infusions because they are not very helpful. On the other hand, we see rapid improvement in symptoms and get early remission (i.e., no further neurologic degeneration). The focus on the CNS is a waste of time because treating the obvious peripheral problems directly avoids unnecessary expense and is much more productive in overcoming the disease.
My treatment strategy for MS stands out for its safety, efficacy, speed and low cost, compared to the standard treatments which are designed to work through the CNS, but it doesn’t impress. I don’t like the DMTs and infusions because they are not very helpful. On the other hand, we see rapid improvement in symptoms and get early remission (i.e., no further neurologic degeneration). The focus on the CNS is a waste of time because treating the obvious peripheral problems directly avoids unnecessary expense and is much more productive in overcoming the disease.
My MS treatment protocol evolved after I had treated many Peripheral Neuropathy (PN) cases. My first MS patient had the standard MS treatment elsewhere and his biggest complaint was numbness from his knees down to his feet for over ten years. At first I considered that he had Peripheral Neuropathy (PN) but his overall clinical picture suggested MS. And because of the similarity between MS and PN I thought I’d see how his MS would respond to my PN treatment. His leg numbness was gone at the end of his first treatment and his legs began to feel stronger. His symptoms continued to improve with each treatment. His myelin sheath areas posed no problem either. His responses suggested that MS is likely to be a peripheral or mixed neuropathy. My treatment is so well tolerated that it allows for longer treatments to get as much improvement as possible per visit.
While the CNS can be involved, peripheral and general symptoms are more common and these can prevent mobility. I prefer to begin with the mobility problems so as to get the patient ambulatory as soon as possible. Then I’ll treat other patient preferential areas. But overcoming pain and immobility are high on the patient’s preference list.
My approach is for frequent and longer treatment sessions as tolerated, focusing on alleviating the most distressing symptoms first, usually mobility or function difficulty. The Dextrose solution is injected beside the nerve without impaling it. This direct approach produces quicker results and the patients enjoy the fast recovery.
Patients who have lived with MS symptoms for years, initially question their potential for recovery, but they find more hope and relief from this treatment. MS nerves have a low glucose level, and near nerve injections raise the nerve glucose to normal. This must occur in order for the nerves to recover their function as quickly as possible. The standard neurological treatments don’t do this most important component for recovery. We’ve discovered that neuropathic nerves, even those dormant for years and seemingly beyond repair, can often regenerate quickly and return to normal.
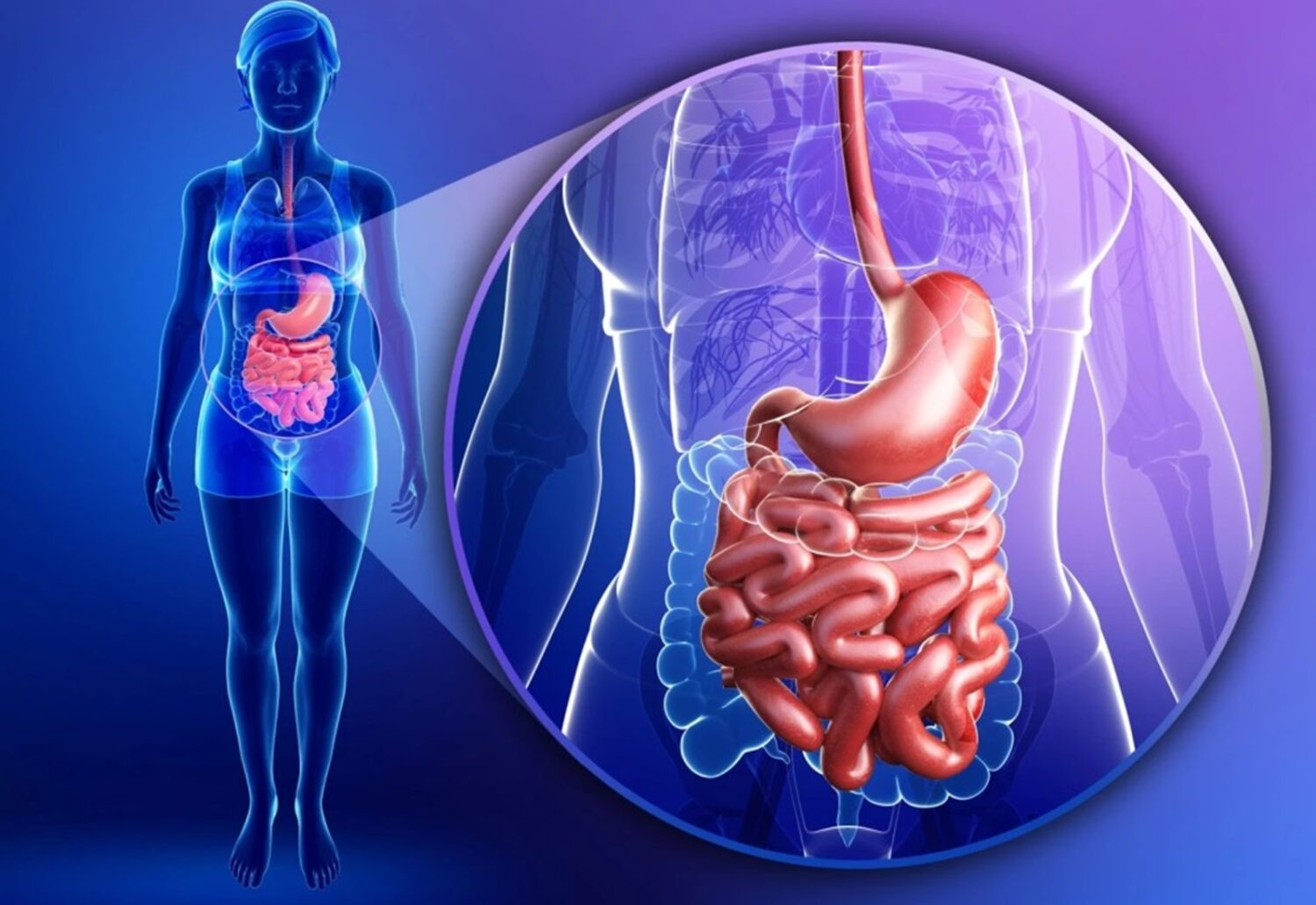 I discovered the cause of Crohn’s disease to be neurologic, similar to Trigeminal neuralgia and Migraine. I had treated these neurological conditions many times previously with dilute dextrose according to the Lyftogt technique of near-nerve injection, and there was always a rapid disappearance of pain. The cause of Crohn’s is a defective glycolysis (a process of converting glucose to energy for nerve function) in the nerves to the intestine. Dilute dextrose promptly normalizes the nerve and the glycolysis ceases to exist. (That’s another example of an abnormal nerve causing the disease; they all appear normal. Other examples: Migraine, dry eye, Glaucoma, etc). I’ve never seen a recurrence of Crohn’s. None of my Crohn’s patients had to have surgery; their pain was gone within a minute.
I discovered the cause of Crohn’s disease to be neurologic, similar to Trigeminal neuralgia and Migraine. I had treated these neurological conditions many times previously with dilute dextrose according to the Lyftogt technique of near-nerve injection, and there was always a rapid disappearance of pain. The cause of Crohn’s is a defective glycolysis (a process of converting glucose to energy for nerve function) in the nerves to the intestine. Dilute dextrose promptly normalizes the nerve and the glycolysis ceases to exist. (That’s another example of an abnormal nerve causing the disease; they all appear normal. Other examples: Migraine, dry eye, Glaucoma, etc). I’ve never seen a recurrence of Crohn’s. None of my Crohn’s patients had to have surgery; their pain was gone within a minute.
The first patient was a 53 yr old female who had Crohn’s since she was 7 yrs old; she had approximately an 8 out of 10 abdominal pain prior to treatment, but her pain rapidly subsided in 20 seconds (I timed it), proving the neurogenic origin of her lifelong struggle with Crohn’s. The injection turned off the cause of Crohn’s rather than trying to oppose the pain. This fantastic relief of Crohn’s occurred first in my office in 2017, and it’s been successful in every case ever since. The treatment is inherently safe, with no known side effects. No Crohn’s patient has to have surgery now.
 My approach to treating migraine represents a significant advancement over traditional methods, offering a safer and more effective solution. We recognize migraine as one form of neuropathic pain, which is notably resistant to standard analgesics because these medications fail to address the underlying cause: a deficiency of glucose within the nerve (neuroglycopenia) caused by a defect in glycolysis (the conversion of glucose to energy).
My approach to treating migraine represents a significant advancement over traditional methods, offering a safer and more effective solution. We recognize migraine as one form of neuropathic pain, which is notably resistant to standard analgesics because these medications fail to address the underlying cause: a deficiency of glucose within the nerve (neuroglycopenia) caused by a defect in glycolysis (the conversion of glucose to energy).
Our technique involves the administration of micro-injections close to the painful areas, a near-nerve injection. Remarkably, this usually results in the cessation of a migraine attack within a few minutes. The patient discontinues their usual migraine medicine the day before treatment. They receive two treatments (about 2 hours apart) the first day and one treatment the next day if needed. Then they won’t ever need another treatment for Migraine. They should avoid high doses of opioids or it could block the treatment.
 My treatment strategy is deeply rooted in the principles of nerve regeneration.
My treatment strategy is deeply rooted in the principles of nerve regeneration.
My approach to treating Trigeminal Neuralgia involves the precise administration of micro-injections of buffered dextrose solution to target the Trigeminal nerve and it’s branches. I place the dextrose between the subcutaneous layer and the nerve. It will soak into the nerve quickly at that level, reducing inflammation around the nerve and eliminating the pain. It’s usually a permanent fix.
 Our methodology for addressing Tennis Elbow involves the precise application of near nerve injections, administering a dilute buffered dextrose solution beside the radial nerve branches (near-nerve injs). This treatment should turn off the pain and inflammation in the elbow and forearm. This should restore strength and normal function to the elbow region, enabling patients to return to their normal activities earlier than standard treatments.
Our methodology for addressing Tennis Elbow involves the precise application of near nerve injections, administering a dilute buffered dextrose solution beside the radial nerve branches (near-nerve injs). This treatment should turn off the pain and inflammation in the elbow and forearm. This should restore strength and normal function to the elbow region, enabling patients to return to their normal activities earlier than standard treatments.
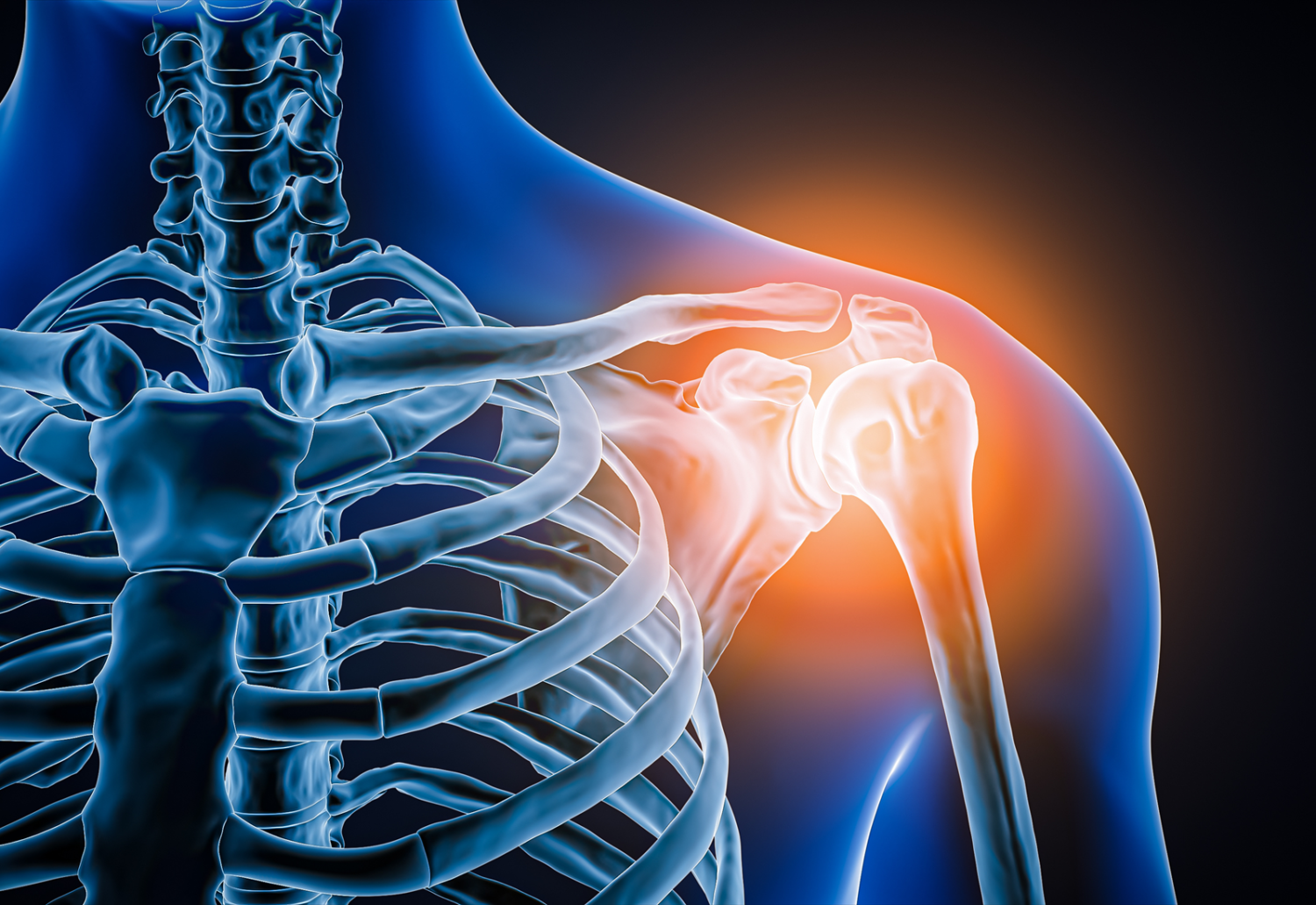 The goal of treating a rotator cuff injury involves finding the precise location of the pain, and then delivering the solution directly to that area to turn off the pain and inflammation. This requires caution to avoid injecting the nearby plexus nerves. The pain usually subsides immediately and healing of the rotator cuff is automatic.
The goal of treating a rotator cuff injury involves finding the precise location of the pain, and then delivering the solution directly to that area to turn off the pain and inflammation. This requires caution to avoid injecting the nearby plexus nerves. The pain usually subsides immediately and healing of the rotator cuff is automatic.
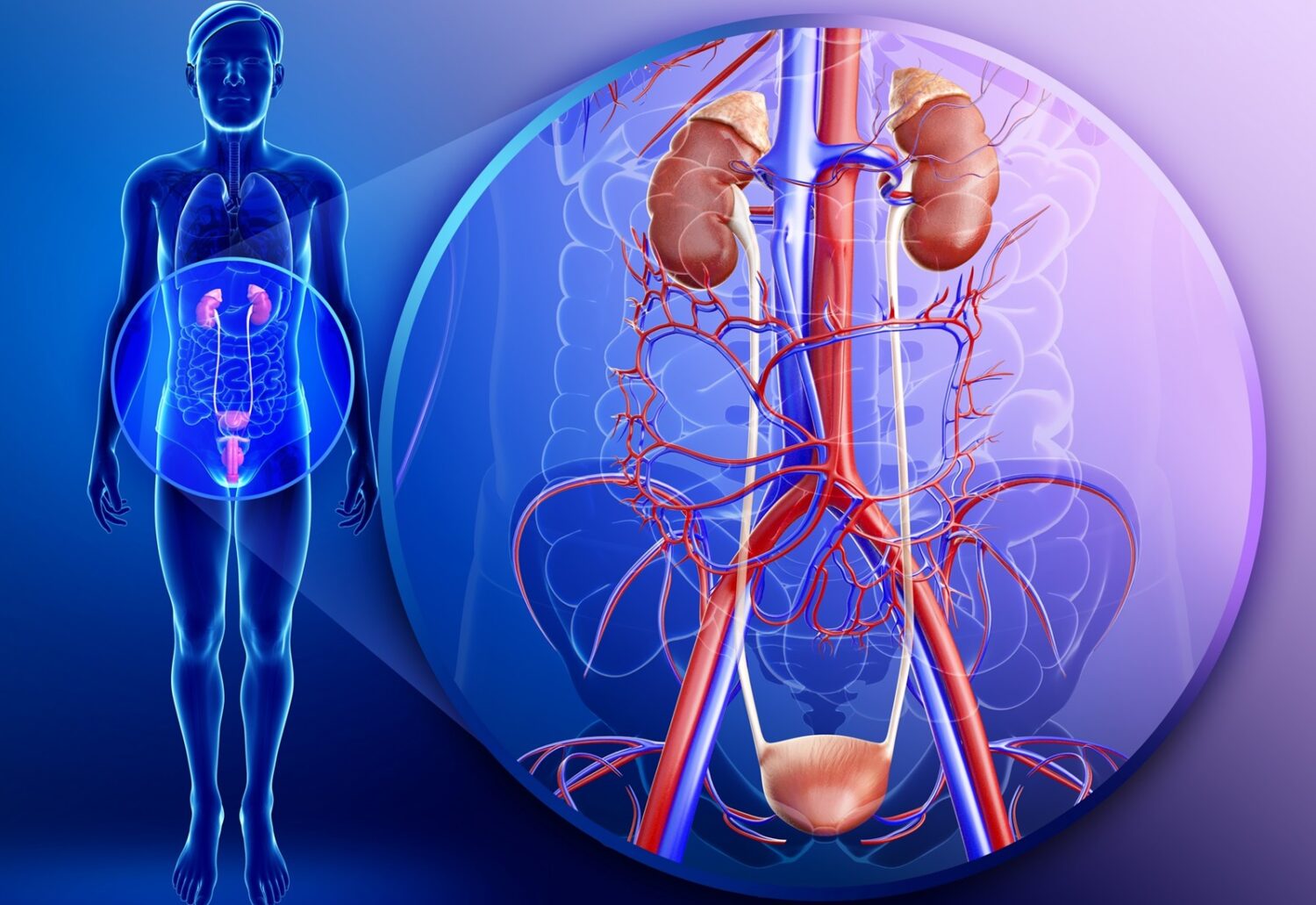 Incontinence can significantly impact quality of life in both men and women. Dr. McDonagh sees this condition as a neuropathy of the autonomic nerves if the urologic evaluation (urinalysis) is otherwise normal. This treatment involves “near nerve” injections to the obturator nerve in the upper thighs, and the dilute dextrose normalizes the nerves. This is a painless procedure.
Incontinence can significantly impact quality of life in both men and women. Dr. McDonagh sees this condition as a neuropathy of the autonomic nerves if the urologic evaluation (urinalysis) is otherwise normal. This treatment involves “near nerve” injections to the obturator nerve in the upper thighs, and the dilute dextrose normalizes the nerves. This is a painless procedure.
 Neuropathic pain can be mild or intense. Peripheral neuropathy involves both motor and sensory nerves, and usually begins with numbness in in the feet. It appears first in the longest nerves and so my treatment begins in the feet. This is important because driving a car with numb feet can be dangerous when you can’t feel the pedals. The good news is that the numbness can usually be treated effectively using “near nerve injections” of buffered dilute dextrose solution. Many of these pts with numb feet may require several foot treatments before the numbness declines. This maybe because the disease begins in the feet (longest nerves affected first). Our entire nervous system including our brain, spinal cord, and peripheral nerves all use glucose for normal function of their motor and sensory nerves. In Peripheral Neuropathy, the first sign of low nerve sugar levels is numbness in the feet. After foot numbness, balance problems becomes more obvious, because the nerves of proprioception (just proximal to the ankle joint) become affected. Next is shooting pains below knee.
Neuropathic pain can be mild or intense. Peripheral neuropathy involves both motor and sensory nerves, and usually begins with numbness in in the feet. It appears first in the longest nerves and so my treatment begins in the feet. This is important because driving a car with numb feet can be dangerous when you can’t feel the pedals. The good news is that the numbness can usually be treated effectively using “near nerve injections” of buffered dilute dextrose solution. Many of these pts with numb feet may require several foot treatments before the numbness declines. This maybe because the disease begins in the feet (longest nerves affected first). Our entire nervous system including our brain, spinal cord, and peripheral nerves all use glucose for normal function of their motor and sensory nerves. In Peripheral Neuropathy, the first sign of low nerve sugar levels is numbness in the feet. After foot numbness, balance problems becomes more obvious, because the nerves of proprioception (just proximal to the ankle joint) become affected. Next is shooting pains below knee.
The nerves in PN can deteriorate to a state of dormancy and can remain in that state for decades, and surprisingly they can regenerate from dormancy in many cases under the influence of repeated dextrose injs. But nerves can die if their environment becomes toxic (from Chemo and Radiation) or there is ongoing damage to the nerve (e.g., compression, trauma, inflammation). Additionally, some patients have cold feet and legs from peripheral vascular disease (poor circulation) which could make PN more difficult to regenerate. There is hope for long standing neuropathy because the nerves can return from dormancy after many years. Serial trials of Dextrose is the best option.
Some patients get peripheral neuropathy from chemotherapy and radiation which can be too toxic to peripheral nerves. These patients should get early dextrose treatment or their nerves could lose their function permanently. Such patients can also develop “dropped foot” on one or both sides. Fortunately this paralyzing problem can be corrected if caught in time.
Peripheral neuropathy can occur anywhere on the body. Neuropathic pain can be felt in neuralgias or pinched nerves (e.g., carpal tunnel syndrome), or as Fibromyalgia., even in back pain commonly caused by the Cluneal nerves (Superior, Middle and Inferior). I also consider MS & ALS to be peripheral neuropathies because of its prompt response to Dextrose. They all respond well to the same dextrose solution technique but the injection methods can vary. Please note that giving dextrose by IV/IM/Orally etc, can’t work because the glucose can’t get to the target area concentrated enough. Also, the Dextrose solution can’t affect the patient’s blood sugar very much because of the low concentration and small volumes of dextrose injected.
 Our treatment for Stiff Person Syndrome focuses on targeted therapy designed to modulate the nervous system’s response. The treatment employs micro-injections of buffered Dextrose, which quickly stops the muscle spasms in the affected areas. Large muscle spasticity can be a painful malady, hindering mobility.
Our treatment for Stiff Person Syndrome focuses on targeted therapy designed to modulate the nervous system’s response. The treatment employs micro-injections of buffered Dextrose, which quickly stops the muscle spasms in the affected areas. Large muscle spasticity can be a painful malady, hindering mobility.
 Carpal Tunnel Syndrome responds well to “near nerve” Dextrose injections. The Median nerve is most commonly compressed by Struthers Ligament about an inch and a half above the medial elbow and again when passing between the two heads of the Pronator Teres muscle.
Carpal Tunnel Syndrome responds well to “near nerve” Dextrose injections. The Median nerve is most commonly compressed by Struthers Ligament about an inch and a half above the medial elbow and again when passing between the two heads of the Pronator Teres muscle.
The “near nerve” injections should begin at these two sites and over any other median nerve tenderness in the forearm including just proximal to the Flexor Retinaculum. This could save you an operation!
The Mayo Clinic published an article on the Dextrose treatment of Carpal Tunnel Syndrome in 2017, comparing it favorably to other injection treatments including effective long term results. The pain & weakness usually fades fast within a few minutes.
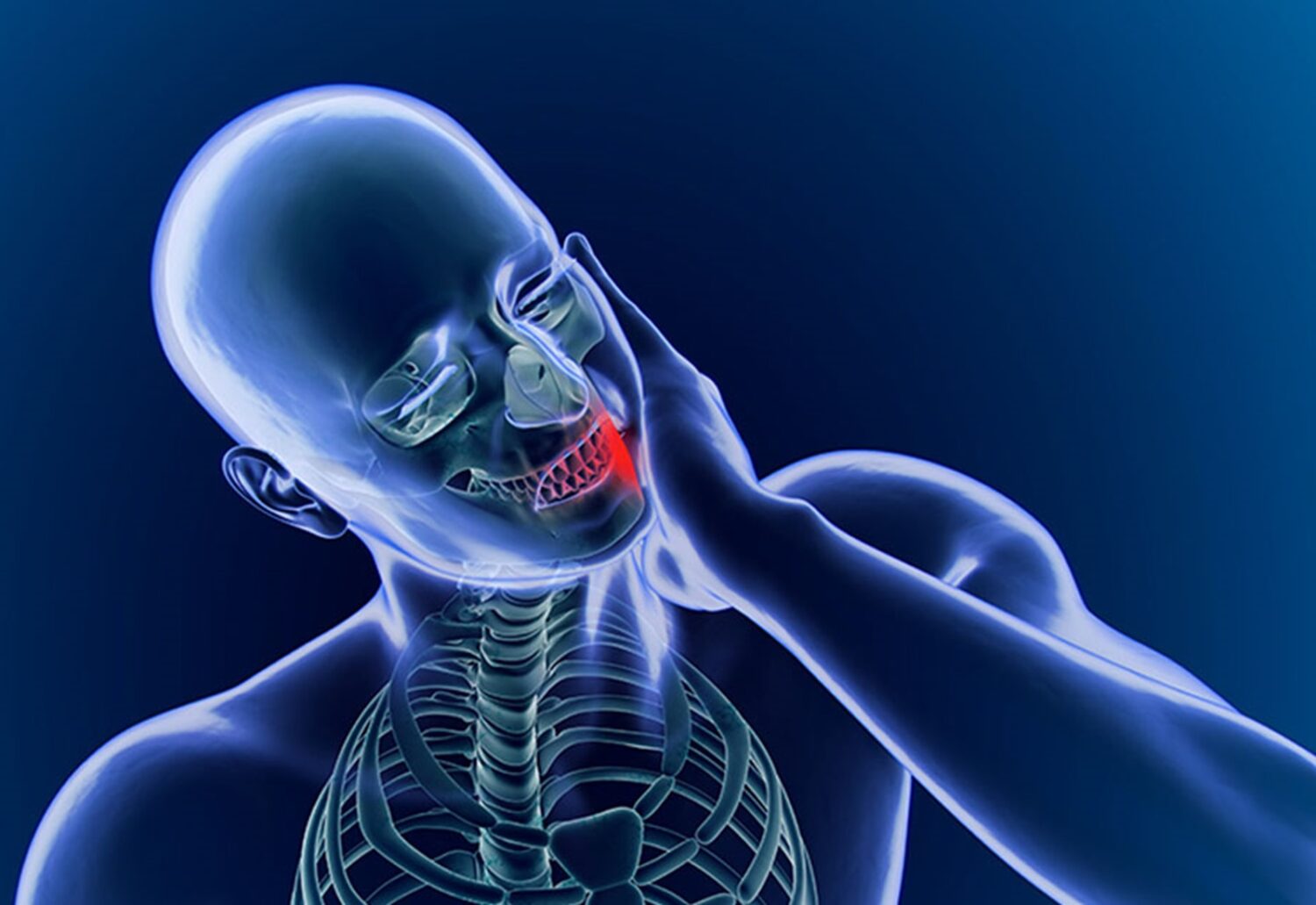
 I enjoy treating painful necks with reduced range of motion, because they respond so well to minimally invasive injections. The nerves from the neck frequently go down through the trapezius muscles and out to the shoulder joints, where they can cause frozen shoulder, which is also a rapid responder to micro injection treatment.
I enjoy treating painful necks with reduced range of motion, because they respond so well to minimally invasive injections. The nerves from the neck frequently go down through the trapezius muscles and out to the shoulder joints, where they can cause frozen shoulder, which is also a rapid responder to micro injection treatment.
Necks that have a reduced range of motion limited by pain are rapid responders to PIT. This is a favorite treatment of patients.